The Bipolar IN Order approach makes claims about what is possible for people with bipolar disorder that go beyond what the standard treatment literature describes. For those claims to be taken seriously — by individuals considering the program, by clinical partners, and by insurance organizations evaluating coverage decisions — they need to be supported by evidence.
This article describes the outcomes evidence that exists, what it shows, and where the research is heading.
The Challenge of Measuring Bipolar IN Order Outcomes
Standard clinical outcome measures for bipolar disorder are designed to capture the absence of symptoms: hospitalization rates, episode frequency, severity scores, medication adherence. These are appropriate measures of the goals of standard treatment.
The Bipolar IN Order framework aims at a different set of outcomes: increasing functionality during episodes, expanding the comfort zone over time, reducing fear and suffering associated with the condition, and developing a qualitatively different relationship to the states themselves.
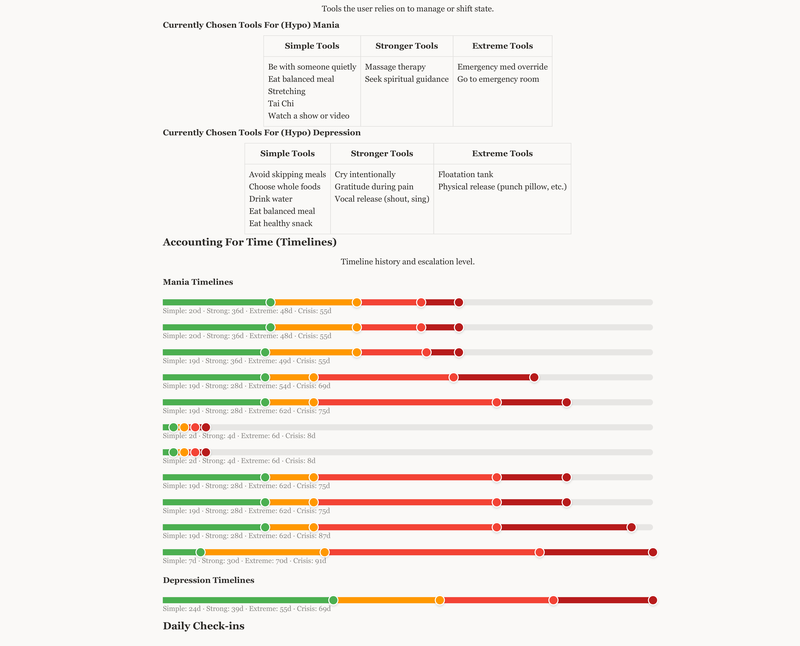
Measuring these outcomes requires different instruments than the standard clinical toolkit provides. The program has developed its own assessment frameworks — measuring functionality across the six dimensions (physical, mental, emotional, spiritual, social, and career/financial) at multiple intensity levels — and uses these to track progress over time.
What Participants Report
Across the participants who have completed Bipolar IN Order courses and intensives, several consistent patterns appear in self-reported outcomes:
Increased functionality during difficult states. The majority of participants who engage seriously with the program report meaningful improvement in their ability to maintain work, relationships, and daily functioning during depressive and elevated states, compared to before the program.
Reduced fear of future episodes. A consistent finding is reduced anticipatory anxiety around future cycles. Participants who have built genuine skills report feeling significantly less afraid of what the next episode might bring — because they have accumulated evidence that they can navigate difficult states without total loss of functioning.
Improvement in relationship quality. Participants in committed relationships frequently report improvement in those relationships as a secondary outcome of the work — not because the program is a relationship program, but because the same skills that improve state management also improve behavioral consistency and the ability to be present for others.
Reduced hospitalization. Among participants who had a history of hospitalizations, many report significant reduction or elimination of hospitalizations following sustained engagement with the program.
The Research Foundation
The broader research context for the Bipolar IN Order approach draws on several streams of evidence:
NIMH STEP-BD findings — The largest study ever conducted on bipolar disorder found that standard treatment, while valuable, leaves a significant portion of participants with ongoing recurrent episodes and functional impairment. This is the baseline against which the IN Order approach is positioned.
Research on functional outcomes — Growing literature on the distinction between symptomatic recovery and functional recovery in bipolar disorder supports the program's emphasis on functionality measurement. Studies show that people can achieve symptomatic remission while remaining significantly functionally impaired — and that functional improvement is a distinct and important treatment target.
Peer support and self-management research — Evidence for the value of structured self-management programs and peer support in serious mental illness has grown substantially. The Bipolar IN Order program shares important features with evidence-based self-management approaches.
What We Are Working Toward
The Bipolar IN Order program is committed to building a more rigorous evidence base for its outcomes. This includes developing standardized measurement tools, creating frameworks for documenting outcomes that can be compared across participants and over time, and pursuing formal research partnerships.
For individuals, families, and clinical partners evaluating the program, the honest current answer is: the evidence is promising and consistent with clinical plausibility, and the formal research infrastructure to demonstrate it at clinical scale is under development.